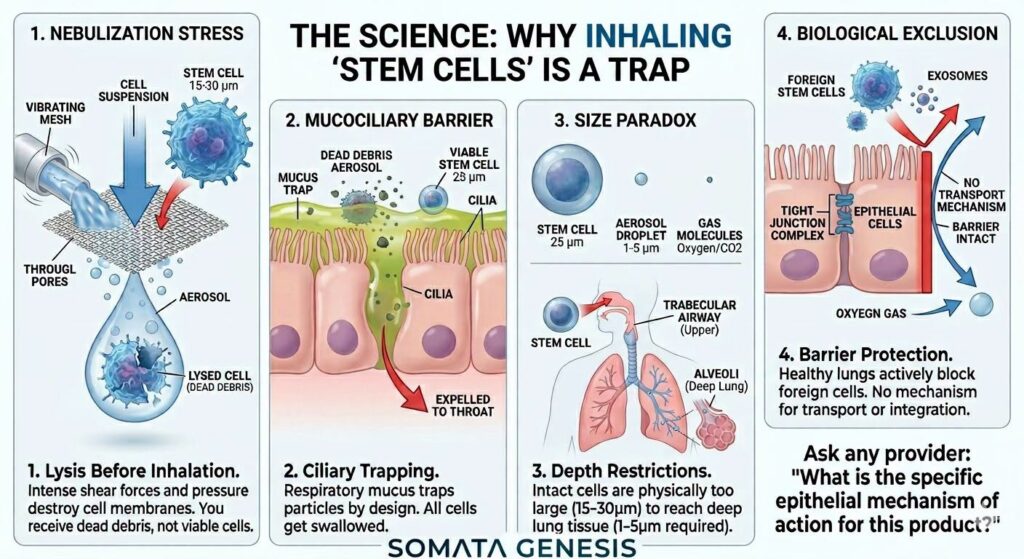
Recent trends in unregulated regenerative medicine have seen the emergence of “spa” clinics marketing the intranasal administration or nebulization of live stem cells—predominantly mesenchymal stem cells (MSCs)—and their derived extracellular vesicles (EVs/exosomes). This paper deconstructs the biophysical, mechanical, and physiological barriers that render these delivery modalities fundamentally unviable. We demonstrate that the shear stress of nebulization rapidly diminishes cell viability, creating an aerosol consisting largely of pro-inflammatory cellular debris. Furthermore, we analyze the physical constraints of the mucociliary escalator, epithelial tight junctions, and the particle size paradox governing respiratory deposition. This analysis confirms that intact eukaryotic cells cannot navigate the respiratory architecture to achieve targeted or systemic therapeutic efficacy.
1. INTRODUCTION
The therapeutic paradigm of cellular biologics relies on the delivery of viable, characterized cell lines to specific target tissues to exert immunomodulatory or regenerative effects. While intravenous, intrathecal, and direct localized injections have established clinical frameworks, the exploitation of alternative routes—specifically inhalation and intranasal delivery—has proliferated in unscientific contexts. Marketing narratives claim these pathways offer a non-invasive conduit to the central nervous system or the lower respiratory tract. However, these assertions ignore fundamental laws of fluid dynamics, aerosol physics, and respiratory physiology.
2. MECHANICAL SHEAR STRESS AND THE HOMOGENIZATION PHASE
The primary biophysical barrier to cellular nebulization occurs during aerosol generation. Whether utilizing jet, ultrasonic, or vibrating mesh nebulizers, the process requires forcing a liquid suspension through microscopic apertures or subjecting it to high-frequency acoustic energy to create breathable droplets.
Eukaryotic cells, lacking a rigid cell wall, depend on a delicate lipid bilayer maintained by a complex cytoskeleton. When subjected to the rapid pressure drops, localized thermal spikes, and intense hydrodynamic shear forces inherent to nebulization, these structures fail.
[Cell Suspension] ──> [Nebulizer Mesh / Orifice] ──> [High Shear & Pressure Drops] ──> [Cell Lysis & Genomic DNA Release]
Rather than generating a therapeutic mist of living cells, the process acts effectively as a cell homogenizer. The resulting output is primarily a lysate composed of:
- Denatured membrane fragments
- Spilled intracellular proteins
- Free genomic DNA
When inhaled, this uncharacterized cellular debris risks triggering localized inflammatory cascades via damage-associated molecular patterns (DAMPs), compounding patient risk rather than offering a therapeutic benefit.
3. THE MUCOCILIARY ESCALATOR AND ANATOMICAL EXCLUSION
For the fraction of cellular products that survive aerosolization or are introduced directly into the nasal cavity, the upper respiratory tract’s primary defense mechanism poses an insurmountable barrier.
The respiratory epithelium is permanently coated in a complex, viscoelastic mucus gel matrix composed of mucin glycoproteins (MUC5AC and MUC5B). This matrix evolved specifically to trap foreign particulates, pathogens, and environmental debris.
Particle Capture Ratio is proportional to Particle Diameter / Pore Size of Mucus Matrix.
Because living cells and large macromolecules possess significant physical mass relative to gas molecules, they undergo rapid impaction and immobilization within this sticky gel. Once trapped, the underlying ciliated epithelial cells drive the mucociliary escalator, continuously sweeping the mucus layer cranially toward the pharynx. The trapped material is subsequently swallowed, exposing the “therapeutic” product to gastric acid and enzymatic digestion in the gastrointestinal tract.
4. THE PARTICLE SIZE PARADOX IN RESPIRATORY DEPOSITION
To achieve deep lung deposition—specifically reaching the alveoli for systemic cross-talk or localized lower respiratory therapy—aroscopic particles must adhere to strict aerodynamic diameter D(ae) profiles:
Aerodynamic Diameter (Dae) — Primary Deposition Site — Dominant Physical Mechanism
>10 μm — Nasopharynx / Upper Airways — Inertial Impaction
5−10 μm — Tracheobronchial Tree — Impaction / Gravitational Sedimentation
1−5 μm — Alveoli (Deep Lung) — Gravitational Sedimentation
<1 μm — Alveoli / Exhaled — Brownian Diffusion
This hierarchy reveals a fundamental physical paradox for cellular delivery:
- A standard mesenchymal stem cell (MSC) in suspension exhibits a spherical diameter ranging from 15 to 30 μm.
- Even in a theoretical scenario where a cell survives nebulization completely intact, its physical dimensions would still result in immediate inertial impaction within the upper nasopharyngeal cavity.
- To reach the lower respiratory tract, an aerosol droplet must be smaller than 5 μm, a physical impossibility for an intact eukaryotic cell.
5. EPITHELIAL INCOMPATIBILITY AND THE ABSENCE OF TRANSLOCATION MECHANISMS
The respiratory epithelial lining is defined by highly regulated apical junctional complexes, including tight junctions (composed of claudins, occludin, and zonula occludens) and adherens junctions. These structures maintain strict barrier integrity, permitting the free diffusion of gases while actively restricting the paracellular transport of foreign entities.
Unlike specific chemical entities or highly engineered nanoparticles that exploit explicit receptor-mediated endocytic pathways, foreign cell lines lack a native physiological mechanism to trigger paracellular or transcellular translocation across a healthy epithelial barrier. The barrier is evolutionarily designed to prevent exactly this type of cellular intrusion.
Furthermore, successful aerosolized pharmaceuticals depend on rigid molecular criteria that cellular biologics lack:
Criteria for Viable Aerosolized Medications:
1. Nano-scale or atomized dimensions (< 100 nm to 5 µm carrier droplets)
2. A highly defined, receptor-specific biochemical mechanism of action
3. Chemical stability, preventing degradation or alteration mid-transit
Live cell suspensions violate all three tenets: they are microscale, rely on dynamic and uncharacterized secretome responses rather than single-receptor small-molecule interactions, and physically degrade during delivery.
6. CONCLUSION AND CLINICAL LITMUS TEST
The administration of live cellular therapeutics via intranasal or nebulized pathways represents a fundamental misalignment of bioprocess engineering and respiratory physiology. The combined forces of mechanical lysis, mucociliary clearance, aerodynamic exclusion, and epithelial barrier integrity ensure that no therapeutic delivery occurs to targeted tissues.
To maintain clinical standards and protect patient safety against uncharacterized biological products, providers offering these modalities must be held to a rigorous clinical litmus test:
“What is the precise epithelial mechanism of action of the cellular product being offered, and what in vivo tracking data demonstrate its viable translocation across the respiratory barrier?”
In the absence of reproducible, peer-reviewed pharmacokinetic and pharmacodynamic data confirming intact cellular transport without localized inflammatory induction, these procedures must be classified as biologically non-viable.
By Surjo Banerjee, Senior Neurobiologist
REFERENCES
Bustamante-Marin, X. M., & Ostrowski, L. E. (2017). Cilia and Mucociliary Clearance. Cold Spring Harbor perspectives in biology, 9(4), a028241. https://doi.org/10.1101/cshperspect.a028241
Fröhlich E. (2021). Therapeutic Potential of Mesenchymal Stem Cells and Their Products in Lung Diseases-Intravenous Administration versus Inhalation. Pharmaceutics, 13(2), 232. https://doi.org/10.3390/pharmaceutics13020232
González, H. E., McCarthy, S. D., Masterson, C., Laffey, J. G., MacLoughlin, R., & O’Toole, D. (2023). Nebulized mesenchymal stem cell derived conditioned medium ameliorates Escherichia coli induced pneumonia in a rat model. Frontiers in medicine, 10, 1162615. https://doi.org/10.3389/fmed.2023.1162615
Habiba UE, Sathyanarayanan R, Shamim S, Manian A, Haider A, Sarwar I and Greene DL (2026) Intranasal administration of stem cells and their derivatives for neurological and respiratory disorders: a systematic review of human clinical trials. Front. Aging Neurosci. 18:1834543. doi: 10.3389/fnagi.2026.1834543